
CerFlux Awarded Patent for a Multimodal Tumor “Supermodel”
BIRMINGHAM, Ala. (January 9, 2026) — CerFlux has been awarded U.S. Patent No. 12,518,880 for a method that turns one of cancer care’s hardest moments — when we lose a patient to cancer — into a way to help the next patient. The patent covers a multimodal tumor “supermodel” at the heart of the CerFlux PROPHET™ technology: with consent, it recovers living tumor tissue donated by patients after their passing and reads it to learn why their treatment fell short and what might have worked — knowledge that feeds back into how future cancer drugs are developed, evaluated, and matched to the patients they can help.
Most of what the field knows about whether a cancer drug works comes from clinical trials and treatment. Clinical trials draw from a narrow slice of the patient population. Eligibility rules, distance from trial sites, transportation, caregiving obligations, and the resources that sustained participation demands all shape who is studied, skewing the evidence toward later-stage disease and toward patients near large cancer centers. A trial can therefore come up short even when a therapy genuinely helps. It is a concern CerFlux raises often: when a trial fails, it rarely means a therapy helped no one — only that it didn't help enough patients to reach statistical power. The responders are real, but without a way to identify them in advance, a drug that genuinely works for a definable subgroup can quietly be lost.
“When cancer claims a patient, I see it as a crime scene. But instead of interrogating the perpetrator — the tumor — we bury the evidence.”
The patent opens an unexpected — and deeply human — path around that problem. Patients with cancer are usually considered ineligible to donate organs, because the same disease that defines their illness makes transplantation unsafe. As a result, the chance to learn from their tumors is most often lost.
To address this forensic loophole, the method creates a respectful, consent-based pathway for patients to contribute living tumor tissue after their passing to research aimed squarely at defeating the disease they faced. Because there is no transplant recipient, the very thing that rules out organ donation is exactly what makes the tissue invaluable for study. For many donors, it is a final contribution: a way to keep helping others long after their own fight.
“We need to make sure that the courage and resolve of every patient count in this fight against cancer. And if clues from this can help even one more patient in the future, then that is not only heroic on the part of the original donor but also poetic.”
Just as important is what is collected. The method calls for gathering tissue while it is still living and with its tumor microenvironment (TME) intact — the extracellular matrix, the three-dimensional architecture, the surrounding “neighborhood” of the tumor — and then characterizing that structure rather than discarding it. This reflects a principle at the heart of the science at CerFlux, one the company often illustrates with chocolate-chip cookies and muffins: the cancer cells are the chips, but the batter around them — the microenvironment — frequently decides whether a treatment works. Preserving the batter, not just the chips, is what makes the resulting model faithful to the patient.
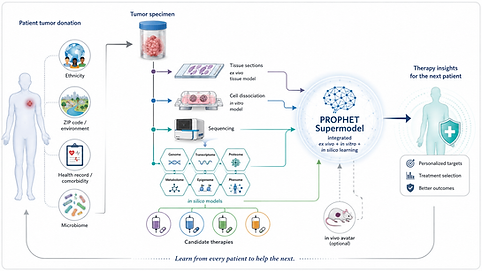
Rather than rely on any single laboratory model, the patented method builds avatars of the same tumor in multiple modalities — in vitro, ex vivo, and in silico (AI/ML) — and weaves them into one integrated picture: a multimodal tumor “supermodel.” At CerFlux, that supermodel is being advanced as PROPHET™. Tissue from a single donor can be split and run in parallel: sequenced for an AI-ready molecular profile, expanded in culture for high-throughput screening against large libraries of drug candidates, and evaluated in tissue-based models that preserve the microenvironment. No single model tells the whole truth about a tumor; the supermodel lets them tell it together, helping surface and prioritize therapies that conventional approaches might miss.
A second advantage comes from where the tissue originates. Because it is obtained post-mortem, the work is not bound to patients who can travel to and sustain participation at a trial site; donors can be far more numerous, and drawn from a far wider range of settings, than typical trial populations. That lets the approach reach beyond the catchment areas of large cancer centers into otherwise remote or under-resourced settings. The same framework supports “counterfactual” analyses: revisiting promising drugs that stumbled in earlier trials, or exploring whether an approved therapy may be a better fit for a particular tumor. De-identified results feed a growing library that can sharpen future AI/ML models and biopharma discovery.
The patent adds to a growing CerFlux IP portfolio and reinforces the CerFlux commitment to human-relevant NAMs and the central aim at CerFlux: getting the right treatment to the right patient, the first time. That goal depends not only on matching a therapy to a tumor, but on a development pipeline faithful enough to human biology that the right therapy survives to exist at all — which is the gap this method is built to help close.